FieldStrength MRI magazine
User experiences - June 2015
University of Bonn is implementing recent techniques in routine in liver imaging after evaluating the added value
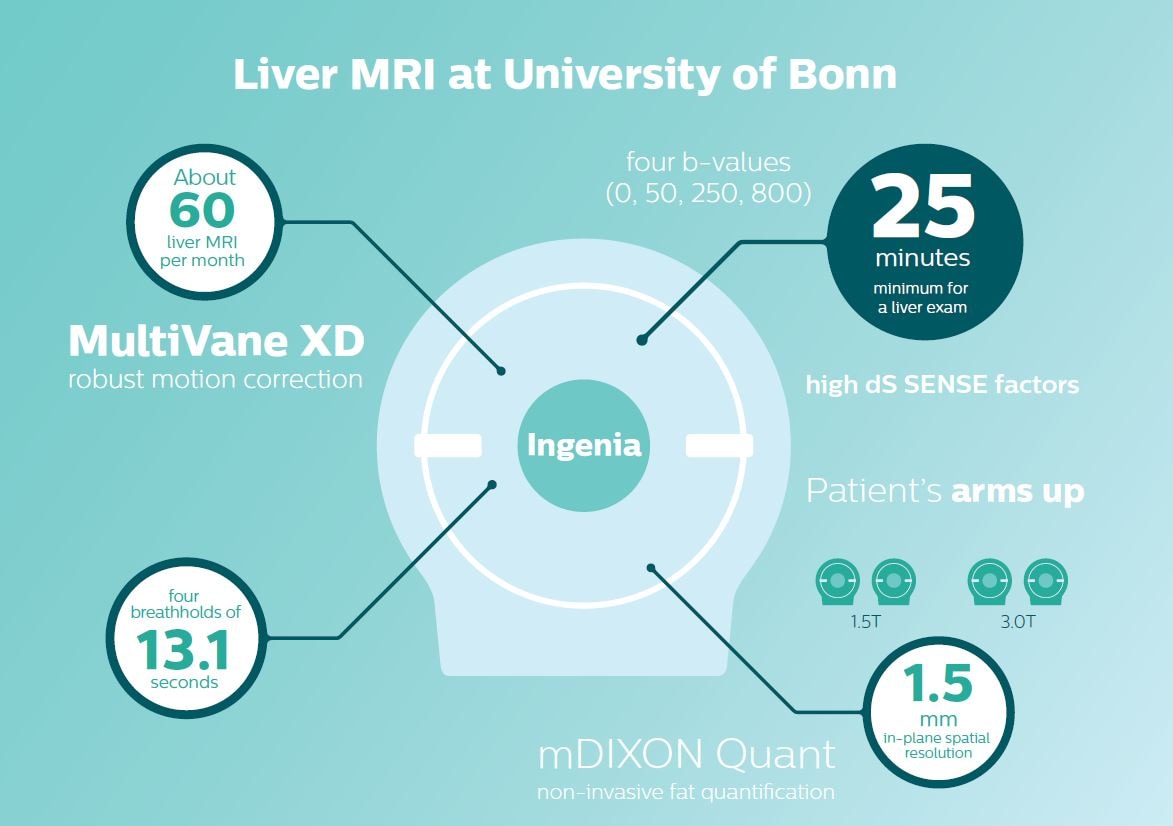
University of Bonn strives for liver imaging that is right the first time and provides sufficient and high quality information for confident diagnosis. Using their Ingenia systems, the team benefits from the dStream digital platform and recently started to use MultiVane XD for robust motion correction and high spatial resolution as well as mDIXON Quant for non-invasive liver fat quantification in just one breath hold.

Guido M. Kukuk, MD is senior radiologist in the Department of Radiology at University of Bonn. He has joined the department in the year 2003 and received his board certification in radiology in 2010. His clinical specialties are abdominal and urogenital imaging.
“The Ingenia system helped us improve the efficiency and image quality of liver exams.”
Ingenia helps improve efficiency and image quality for liver scans
The Department of Radiology at University of Bonn (Bonn, Germany) has two 3.0T and two 1.5T Philips MRI systems. The department performs about 60 liver MRI exams per month, including exams in oncology patients to inform intervention planning and follow-up, scanning of transplant and surgery patients, and outpatient imaging for the department of hepatology. Radiologist Guido M. Kukuk, MD, says the team prefers to use the Ingenia 3.0T and 1.5T systems because of the excellent image quality they provide.
“The Ingenia system helped us to improve the efficiency and image quality of liver exams. Ingenia’s dStream digital coil technology provides increased signal compared to analog Achieva systems, which we see translate to better image quality,” says Dr. Kukuk. “The MultiTransmit technology of Ingenia 3.0T adds the advantage of reducing dielectric shading, which is especially valuable in abdominal imaging.”
“The Posterior coil integrated in the Ingenia patient table is a time-saver,” says Dr. Kukuk. “It allows easy patient positioning and planning and provides high quality imaging. We can obtain a large field of view with both 1.5T and 3.0T systems, which allows us to extend the anatomic coverage when we notice pathology on the first images.”
The need for speed in liver imaging
“Speed is helpful in patients who cannot hold their breath adequately, so it’s desirable to have very fast T1-weighted images. The most important sequence to be fast is the arterial phase, as this sequence cannot be repeated. It has to be first-time-right, really fast and sharp to be diagnostic. I would recommend carefully explaining to the patient before acquisition of this sequence.” “Because we use liver-specific contrast agents, the minimum time we need for a liver exam is about 25 minutes,” adds Dr. Kukuk.

Clinical cases
")
")
A smart examination design
Dr. Kukuk’s liver exam begins with T2-weighted imaging, single shot and with fat suppression. “We always perform diffusion weighted imaging (DWI) with four b-values (0, 50, 250, 800) for lesion characterization, for monitoring after therapies, and for visualization of small lesions. Before giving contrast we routinely use the mDIXON Quant fat quantification sequence. Then we use dynamic e-THRIVE with an in-plane spatial resolution of 1.5 mm and high temporal resolution in just four breathholds of 13.1 seconds.” “Contrast enhancement is important to help us characterize lesions, for follow up in oncology patients and to inform clinicians when deciding on possible changes in the therapeutic regimen,” Dr. Kukuk explains. “Because we use liver-specific contrast agents we can obtain the T2-weighted images after the dynamic, to bridge the waiting time needed with these contrast agents. Just before the patient leaves the scanner we acquire another e-THRIVE in the axial plane and one or two coronals.”
“With the patient’s
arms up, we get faster
scanning and better
image quality.”
“MultiVane XD is a great technique to obtain high spatial resolution T2-weigted images of the liver without relevant motion.”
Imaging with arms up means faster, better imaging
Dr. Kukuk scans an increasing number of liver patients in an arms-up position using the integrated Posterior coil and a special positioning device. “By placing the patient’s arms up, the field of view in the right-left direction can be smaller so that a right-left preparation direction can be used to cut down the scan time,” he explains. “We can use high dS SENSE factors for TSE imaging, so we can shorten the echo train length. This results in a faster scan than arms-down T2 TSE and the images show high anatomical detail.”
“For DWI, the high dS SENSE factor allows using a shorter TE so we get higher signal and fewer susceptibility artifacts, which means less distortion of diffusion weighted images. Of course, with higher dS SENSE factors and the shortening of the TSE factor in T2-weighted imaging, we can drastically cut down the complete examination time. So, with arms-up we get faster images, less distortion in DWI and less blurring on T2-weighted images. Almost all patients tolerate the arms-up scanning well.”
Robust motion correction and high spatial resolution with MultiVane XD
“Using MultiVane XD motion correction, we are now able to acquire high spatial resolution T2-weighted images without seeing relevant motion,” says Dr. Kukuk. “It’s a great technique to obtain high spatial resolution images of the pancreas or the liver, as well as the surrounding organs and tissues. MultiVane XD can be combined with dS SENSE parallel imaging, allowing us to reduce specific absorption rates (SAR), acquire high spatial resolution in short acquisition times, and at the same time reduce artifacts caused by motion in adjacent tissues and organs.”
“In comparison to single shot T2-weighted TSE, this approach with MultiVane XD motion suppression provides higher spatial resolution. In addition, it is especially valuable in patients who cannot hold their breath or have some disabilities. My impression is that this sequence has the potential to substitute for, or even replace, the T2-weighted single shot sequence in our liver exams, because of good and consistent delineation of small lesions.”
“I would recommend acquiring mDIXON Quant liver fat assessment routinely in liver MRI exams as it is fast, easy to use, and has been well evaluated.”
mDIXON Quant is a simple sequence to include in routine liver MRI
“We have performed a study comparing mDIXON Quant fat percentages with results from histopathology. The correlation with different histologic methods was very good and also the correlation with MR spectroscopy was far above 0.9 – a nearly perfect correlation,” says Dr. Kukuk.
“So, this fast mDIXON Quant sequence allows us to diagnose, quantify, and follow up – that’s the real advantage. Our gastroenterologists were easily convinced, as they are well aware of the limitations of ultrasound and the risks of liver biopsy.”
“Also patients appreciate receiving the quantitative diagnosis and changes seen in follow-up exams during therapy.”
“I would recommend acquiring mDIXON Quant routinely in liver MRI exams. It is fast, easy to use, and has been well evaluated [2,3]. The time investment is low and the benefit is high.”
Non-invasive liver fat quantification in a breathhold with mDIXON Quant
“Fatty liver disease is a common condition. Studies found a prevalence of non-alcoholic fatty liver disease in up to 44% in the general European population [1]. Liver fat cannot be quantified by ultrasound or CT, so biopsy has been the way to quantify fatty liver disease so far,” says Dr. Kukuk. “mDIXON Quant now allows non-invasive quantification of liver fat, which is valuable for both diagnosis and follow-up during dietary changes or therapy, for instance in hepatitis C.”
“The mDIXON Quant fat fraction maps provide quantitative information and also anatomical detail. The sequence is fast, usually taking about 16 seconds, which is just a breath hold for most patients. It definitely improves our efficiency.”
“We get fast images, less distortion in DWI and less blurring on T2-weighted images.”
References
1. Blachier M, Leleu H, Peck-Radosavljevic M, Valla DC, Roudot-Thoraval F. The burden of liver disease in Europe: a review of available epidemiological data. J Hepatol 2013; 58: 593-608
2. Reeder SB, Cruite I, Hamilton G, Sirlin CB. Quantitative assessment of liver fat with magnetic resonance imaging and spectroscopy. J Magn Reson Imaging 2011; 34(4): 729-49
3. Yokoo T, Browning JD. Fat and iron quantification in the liver: past, present, and future. Top Magn Reson Imaging 2014;3(2):3-94
Results from case studies are not predictive of results in other cases. Results in other cases may vary.
Results obtained by the facility described in this article may not be typical for all facilities.